Newsletters
The header image is the default header image for the site.MCI Preparedness
POSTED: June 25th, 2024
POSTED IN: 2024 Quarter 2, EM Pulse - The Official Newsletter of MOCEP,
By Erica Carney, MD, Kansas City Office Of The EMS Medical Director
Writing this article is certainly one of the toughest things I have written so let’s get into it, but before we start let’s review some quick definitions to align concepts.
What is the definition of a “mass gathering”? Some say “> 1,000 persons.” Most published data quotes > 25,000 persons. FEMA uses “special events,” which represents a non-routine activity that brings together a large number of people. This is with emphasis on communities’ ability to respond and the exceptional demands placed on services. WHO says, “any occasion that attracts a sufficient number of people to strain planning and response resources.” These definitions help when planning for geographical differences, and/or declaring a disaster to bring in outside resources.
For us working in the inner city, our resources are strained already. We care for multiple shootings a week, so what is the definition of a Mass Casualty Incident (MCI)? For us, a common definition may sound like “unique challenges added to an already taxed EMS systems, hospital systems, transportation systems, and law-enforcement agencies all included”. In studying MCIs, it has been found that certain risk factors can more commonly escalate a mass gathering into an MCI. These include crowd disturbance, fire, structural collapse, natural disaster, disease outbreak, and terrorist attack. Most recently – ballistic.
A final definition to understand is what is a declared disaster? A disaster has been defined as when a natural or man-made event causes overwhelming loss of life, injury, destruction of property or loss of infrastructure. Reviewing EMS Fellowship training and Emergency Medicine training for a disaster is not uniformly required nor standardized.
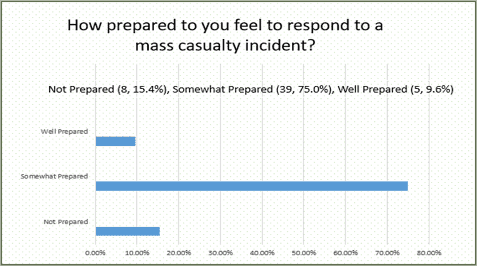
To help our facility obtain a baseline level of mass gathering, MCI, and disaster knowledge, we conducted a survey. This survey is titled “A Survey to Determine Knowledge of Mass Casualty Policy at a Level-1 Trauma Center.” We deployed a knowledge assessment test using REDCap (https://redcap.umkc.edu/surveys/?s=jjzRkKsH58) to determine the basic knowledge of our hospital’s disaster response plan. Results were 100% anonymous. Count data was analyzed using Chi Squared Test of Association. Continuous data was assessed using independent t-test and ANOVA. All emergency medicine staff physicians and residents responded (n=52). Our emergency medicine residents scored 54.8 ± 13.4 points. Our staff emergency medicine physicians scored 64.5 ± 13.5 points. We found that the training year was not associated with the test score (p=.104), and only 9.6% of physicians (5/52) felt well prepared for a mass casualty event (results below).
Now let’s look at traditional specialists’ training, which helps highlight some deficiencies. Emergency medicine physicians receive the most disaster training of all primary specialties. ACGME does require emergency medicine residents to participate in a disaster and/or MCI drill. Only a small percentage of medical schools include disaster training in their core curriculum. Again, the training is not usually standardized. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) requires accredited hospitals to implement a response plan twice a year.
EMS Physicians and our ACGME Fellowship requirements include more preparation. This includes participating in a mass casualty and/or disaster, developing a mass gathering medical plan, and participating in the implementation of this plan. The EMS physician curricula for most EMS fellowships also includes disaster preparedness and management, learning about the Federal framework based on Presidential Policy Directive 8, learning the National Response Framework (NRF) that describes the emergency support functions, and is aligned with National Incident Management System (NIMS). NIMS defines command and management structures that allow for scalable, multijurisdictional response. A final requirement is learning and practicing Incident Command Structure (ICS), and learning about non-governmental organizations, state/NDMS/DMAT/SEMA abilities, and urban search and rescue. For paramedics, CoAEMSP/CAAHEP has not yet made disaster training a separate requirement and the Disaster Medicine Fellowship remains unaccredited by ACGME.
As an emergency medicine physician, please never self-deploy to an MCI without clear consent from the providers on scene. Less people on the scene helps with overall security and safety. The providers working the event were all able to be tracked, given our preparation.
During the post-event reviews, we found that our responders likely suffered the effects of stress. This is a long-term process. Post-event operational debriefing occurred where areas for improvement were identified. Studies have shown that post traumatic stress symptoms and PTSD will happen. This is the current disposition of many of our affected providers. Constant exposure will occur with interviews, presentations, and awards discussing this event. Therefore, repeat, and organic debriefings are a strong consideration.
At the end of the day, we already have the training and practice to respond to most MCI patients. It’s our day-to-day job. We must make our administrative policies and operational procedures match, and everyone needs a seat at the table.