Newsletters
The header image is the default header image for the site.Weighing the Utility of Serum Lactate in Obese Patients with Sepsis
POSTED: June 19th, 2026
POSTED IN: 2026 EM Pulse Q2, EM Pulse - The Official Newsletter of MOCEP, forum, Forum Topic,
Written by Manoj Arra, MD, PhD, and Christopher Holthaus, MD
Sepsis remains a prevalent but sometimes puzzling disease in emergency departments throughout the world, challenging ER physicians with frequently changing diagnostic criteria, common disease mimics, and financial implications of “appropriate” management. Sepsis is defined as a pathological host response to infection characterized by vital sign abnormalities, organ dysfunction, and ultimately death. It exists on a spectrum from low-mortality disease to high-mortality-shock states. The Surviving Sepsis Campaign (SSC) was founded over 30 years ago as an attempt to improve disease identification and mortality, especially when sepsis progresses to septic shock. Subsequently, a standardized approach to disease treatment was established, composed of early antibiotics, fluid resuscitation, and vasopressors. An important component of sepsis detection involves measurement of serum lactate, a non-specific biomarker that can potentially serve as a measurement of disease severity. Lactate is a cellular metabolic by-product elevated in disease states, often due to multiple causes including inflammation-mediated shifts in metabolism, perfusion, and organ function. However, current sepsis identification and treatment guidelines follow a cookie-cutter, one-size-fits-all approach, such as broadly utilizing a lactate threshold of 2 to help identify patients with sepsis, which may not apply to all patients.
One specific subgroup understudied in the realm of sepsis is obese patients, who often display significant differences in physiology from their non-obese counterparts. ED physicians in Missouri encounter obese patients frequently, with nearly 1 in 3 adults in the state meeting criteria for obesity based on BMI. However, it remains unclear whether obese patients have differences in lactate levels compared to non-obese counterparts, which can influence sepsis diagnosis, identification, and management, especially given the emphasis placed on lactate levels by SSC and CMS. In our study, we measured lactate levels and their efficacy in predicting 30-day mortality in obese and non-obese sepsis emergency department patients at Barnes Jewish Hospital, a large quaternary care center located in St. Louis, Mo. Utilizing a retrospective approach to identify patients with sepsis and manual review to exclude sepsis mimics, we were able to identify 1,442 patients who presented to the ED between 2019 and 2022. These were further separated into obese and non-obese patients, as well as patients requiring vasopressors (shock) and those who did not.
The results displayed that obese patients with sepsis had lower initial lactate levels compared to non-obese counterparts in both non-vasopressor-dependent and vasopressor-dependent sepsis, though they did not display significant differences in mortality (Table 1). Furthermore, lactate had a similar performance as a biomarker for 30-day mortality in obese and non-obese patients when ROC curves were generated (Figure 1). Most importantly, this work highlighted the overall moderate performance of lactate as a predictor of mortality in all subgroups, highlighting the need for improved biomarkers for sepsis identification and prognostication. Based on these findings, it is likely appropriate to continue to use current lactate thresholds for obese and non-obese patients as mandated by CMS, given the small but significant differences. However, there may be some edge cases in which obese patients with sepsis may not be recognized due to borderline lactates (e.g., serum lactate =1.9).
This work was supported by the MOCEP resident research grant. The results from this work were presented at multiple conferences and published in the Journal of Emergency Medicine.
| Table 1a. Non-Vasopressor Dependent Sepsis Patient Characteristics | ||||
| Obese (N=359) | Non-Obese (N=719) | Differences (95% CI) | ||
| First Lactate (mmol/L)- median (IQR)* | 2.2 (1.6, 3.2) | 2.4 (1.6, 3.8) | -0.2 (-0.40, -0.10)* | |
| 30 Day Mortality – n (%) | 31 (8.6) | 70 (9.7) | -1.1% (-4.9%, 2.7%) | |
| Table 1b. Vasopressor-Dependent Sepsis Patient Characteristics | ||||
| Obese (N=87) | Non-Obese (N=277) | Differences (95% CI) | ||
| First Lactate (mmol/L)- median (IQR) | 2.80 (1.80, 5.8) | 3.3 (1.9, 5.6) | -0.5 (-1.2, 1.0) | |
| 30 Day Mortality – n (%) | 21 (24.1%) | 67 (24.2%) | -0.1%, (-10.4%, 10.3%) | |
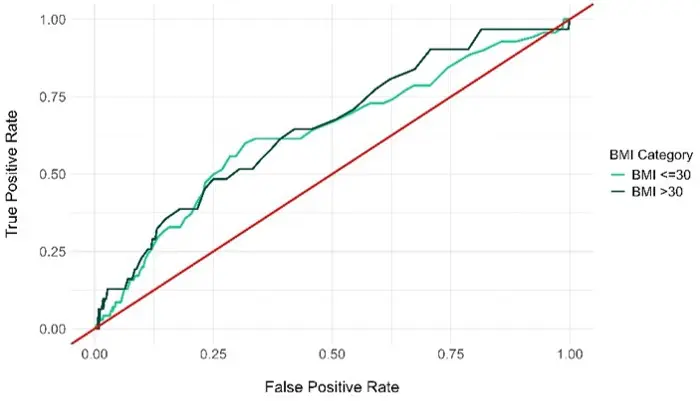
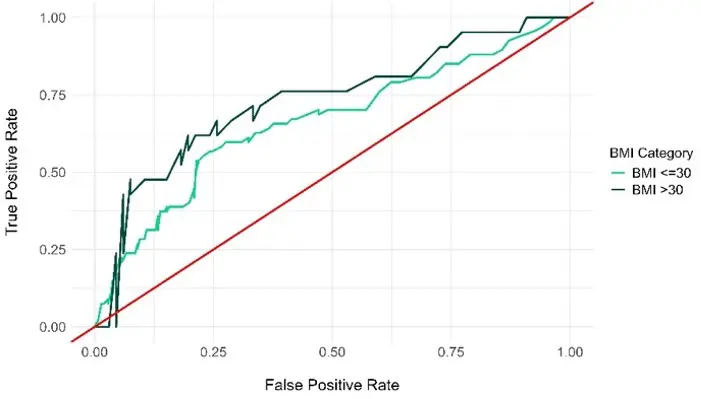
Figure 1a. Unadjusted ROC Curves for Lactate and 30 Day Mortality in Non-Vasopressor Dependent Sepsis Patients by BMI Category (top). Curves generated for obese (AUC=0.65) and non-obese (AUC=0.63) groups. Red line indicates value of 0.5.
Figure 1b. Unadjusted ROC Curves for Lactate and 30 Day Mortality in Vasopressor Dependent Sepsis Patients by BMI Category (bottom). Curves generated for obese (AUC=0.73) and non-obese (AUC=0.66) groups. Red line indicates value of 0.5